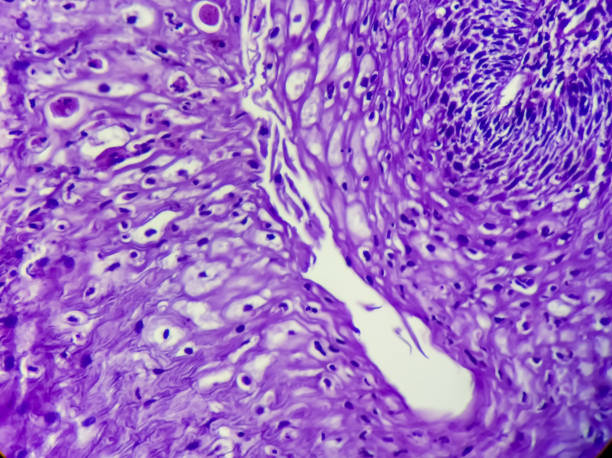
Light Chain Deposition Disease
The patient presented with a history of MGUS and diabetes mellitus. He was subsequently diagnosed with renal failure and proteinuria. His serum kappa/lamda ratio was seven and free kappa was 157 mg/dl. The overall findings of the patient suggest light chain disease with deposition of light chains in the glomeruli. He also presented with long fibrils, which are characteristic of fibrillary glomerulopathy.
What are the symptoms of light chain disease?
Light chain deposition disease is usually a complication of another disease and is much more common in older people. Its symptoms are similar to other deposition diseases, although there are some differences. The other diseases form a pattern in a single section of the kidney, while light chain disease occurs in various parts of the kidney. For this reason, the pathologist studying your biopsy will use a special stain to distinguish it from other deposition diseases.
It can also involve the lungs, but is uncommon. This rare complication usually affects the parenchyma and rarely affects the bronchial tissues. In our case, a 64-yr-old woman presented with a chest CT scan showing diffuse bronchial thickening and two lung cysts. Further, a fibreoptic bronchoscopy revealed a number of nonamyloidal deposits and vascular plexuses in the bronchial wall.
Patients with the disease may experience proteinuria and nephrotic syndrome. A renal biopsy will confirm the presence of light chains in the kidney. About 85 percent of patients with LCDD have deposits of these proteins in the blood and urine. In addition to the kidneys, light chains may also deposit in the heart, liver, small intestine, and skin. Some people may also develop peripheral neuropathy, whereby light chains interfere with a person’s ability to feel pain.
Is there a cure for light chain disease?
Although there is no known cure for light chain deposition disease, treatments are available to help patients manage their symptoms. The disease is a rare condition that typically affects the liver, heart, and kidneys. Patients with the disease often experience nephrotic syndrome, marked proteinuria, and rapid declines in renal function. The disease is more common in men than women. Symptoms of the disease may vary, depending on its cause, but may include muscle weakness, fatigue, weight loss, bone pain, and numbness.
Treatment is centered on treating the underlying causes of the disease. Treatment for light chain deposition disease consists of treating the symptoms, preventing the disease from progressing, and controlling the underlying cause. Bortezomib, a proteasome inhibitor, inhibits the action of NFk’B, which is the cause of pathological changes in glomeruloesclerosis. Bortezomib can be taken along with dexamethasone for light chain deposition disease.
The development of accurate biomarkers for light chain amyloidosis and cardiac biomarkers is improving the prognosis of patients with light chain amyloidosis. These tests allow doctors to identify patients who would benefit from upfront bortezomib combinations. The recent breakthrough in biomarkers is reshaping the way AL amyloidosis is managed.
What causes light chain disease?
Light chain disease is a condition in which the body produces too many of these proteins. They then accumulate in various tissues, including the kidneys, and can overwhelm the kidneys’ recycling capability. Patients often experience symptoms of weakness, fatigue, weight loss, bone pain, and numbness. While it is difficult to predict how patients will progress, some patients have an excellent outcome.
A diagnosis of light chain disease can be complicated by the presence of multiple underlying causes. It is a relatively rare disorder, with a median age of 58 years and a higher incidence among men. The disorder is related to monoclonal gammopathy of renal significance (MGRS), a group of B-cell proliferative diseases that produce monoclonal immunoglobulins in multiple organs, including the kidney.
In light chain disease, the monoclonal immunoglobulins accumulate in the renal parenchyma. These deposits form granular structures. These granules are characterized by cationic polypeptides that bind to anionic basement membranes and lead to deposition. During deposition, mesangial cells act like myofibroblasts, downregulating matrix metalloproteinases and forming a fibrotic matrix. The disease may be accompanied by an underlying MM. In approximately 3% of patients, an autopsy will reveal evidence of light chain disease.
Is light chain disease the same as multiple myelom
Multiple myeloma and light chain disease are different diseases. While both share some symptoms, light chain disease is different in that it causes only light chain plasma cells. In patients with light chain disease, these plasma cells often produce only light chain antibodies. These proteins are excreted in the urine and are used to diagnose and monitor the disease. Physicians use urine protein electrophoresis and urinary immunofixation electrophoresis to identify light chain disease. They also use 24-hour urine collection to measure the amount of protein excreted in the urine. However, recent advances in technology have replaced these urine tests with the Free Light Assay (FLA) to more accurately measure light chains in the blood.
Patients with light chain disease often experience kidney problems due to the buildup of light chain proteins in their blood. The disease’s prognosis is generally less good compared to that of other types of myeloma. Patients with light chain disease should discuss their outlook with their physician and develop an appropriate treatment plan.
How long can you live with light chain disease?
The prognosis for light chain deposition disease is unclear and is linked to other health conditions. Although most patients die within a month of first experiencing symptoms, some patients can live for as long as 10 years. However, the overall prognosis for long-term kidney health is poor. Some people can take measures to slow the progression of the disease. Staying well hydrated is one way to help prevent further damage to the kidneys. A diuretic can also be used to help increase urine output.
The recent advances in the treatment of AL amyloidosis have ushered in significant improvements in survival. However, despite these improvements, mortality rates remain poor. Researchers from the Boston University Amyloidosis Center evaluated mortality rates, primary causes of death, and survival trends in patients diagnosed with the disease. They found that over the past 40 years, the median survival has improved. The percentage of patients who die within six months decreased from 23% to 13%.
When the disease has spread to multiple organs, the prognosis is often poor. The American Cancer Society estimates that the 5-year relative survival rate for multiple myeloma is 75 percent, but that figure drops to 53 percent if the cancer has spread to multiple organs. Light chain myeloma also has a worse prognosis compared to other types of myeloma. It is more likely to cause kidney failure and bone disease. In some cases, the disease can cause the buildup of light chain cells in organs, including the liver.
How long can you live with light chain myeloma?
If you are diagnosed with light chain multiple myeloma, you should know what to expect during your treatment. The outlook is generally poor, as the disease is aggressive and often causes kidney failure. However, with the right treatment, you can expect to live for at least five years.
Treatment is usually aimed at treating the underlying disease. Some treatments can help prevent further kidney damage. These include keeping well hydrated and using diuretics to increase urine output. Patients should also consider a combination of medications. The best option for them will depend on their overall health and their specific symptoms.
The outlook for light chain myeloma patients depends on early diagnosis and treatment. Earlier diagnosis increases the likelihood of cure. However, patients should be aware that the disease can lead to amyloidosis, which affects two or more organs.
How fast does light chain myeloma progress?
In patients with kappa light chain MM, the disease can progress rapidly. It can lead to renal failure, with some patients needing dialysis. Light chains can also deposit in nerve sheaths, causing neurological symptoms. Patients may also develop immunological deficiencies, including decreased levels of antibody proteins, leading to an increased risk of infections.
Patients with light chain MGUS or myeloma secrete protein that is detected by a urine test. The protein, which is called Bence Jones protein, can be used to diagnose and monitor the condition. In patients with non-secretory myeloma, however, the patient’s serum contains little or no immunoglobulin, making the diagnosis more challenging. However, PET-CT scans and bone marrow tests may help diagnose the disease and monitor its progress.
In 2014, a serum free light chain (FLC) ratio of 100 was added to the multiple myeloma (MM) definition. In previous studies, this ratio was associated with an 80% 2-year progression rate and 12-month median time to progression. However, two recent studies have reported lower two-year and four-year progression rates and a longer median TTP. In spite of the disparity in results, the FLC ratio > 100 was added to the definition of MM.
Is light chain myeloma fatal?
Light chain myeloma is a type of cancer that can cause severe kidney damage. It is caused by a buildup of light chain proteins, which are very small. These proteins circulate in the bloodstream and can clog filters in the kidneys. They can lead to permanent damage to the kidneys.
It is more common in African Americans than in Caucasians, and is usually diagnosed through a blood test. Although light chain multiple myeloma is usually fatal, doctors are able to detect it in a person before symptoms appear. In many cases, a person will develop the cancer without symptoms and can be treated with a combination of chemotherapy drugs.
Light chain multiple myeloma is less common than the other types of multiple myeloma. This type of cancer has a worse prognosis than the IgG and IgA subtypes. Although no specific treatment is available for light chain multiple myeloma, the drug Velcade, a first-in-class proteasome inhibitor, has recently been approved by the FDA and the European Medicines Agency (EMA) for treatment of patients with relapsed or refractory disease. In a recent study, researchers looked at the clinical characteristics and responses to therapy in 459 patients with light chain MM.